Hypomineralised Molars

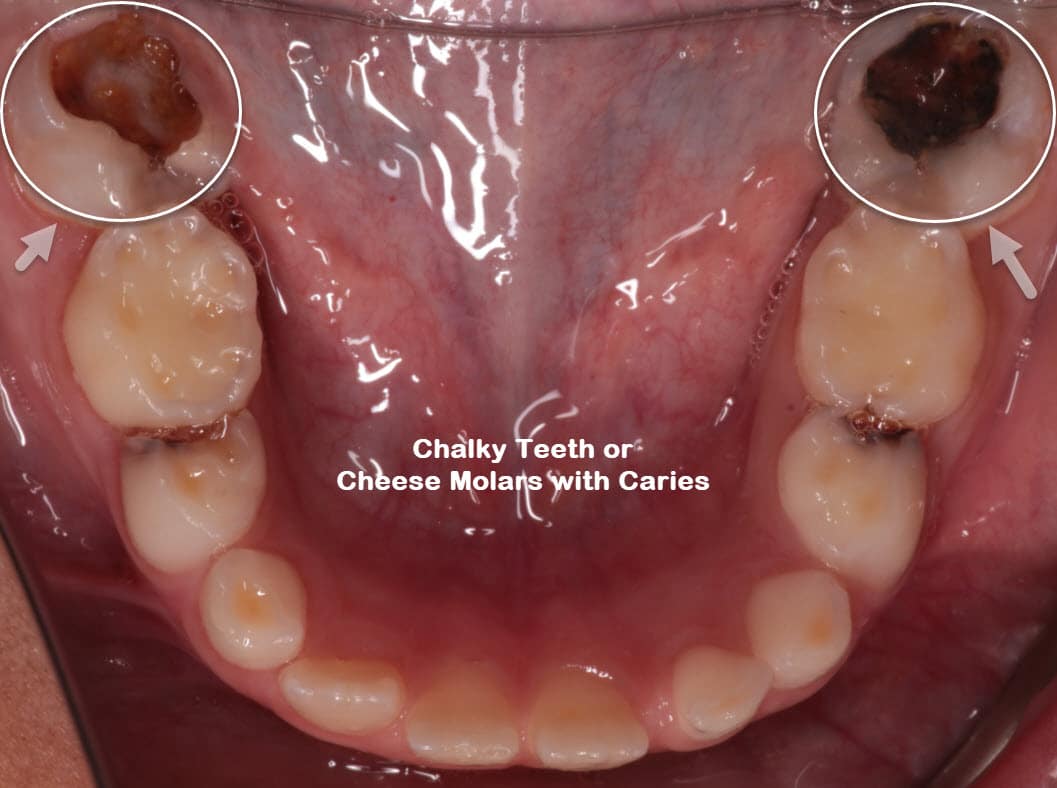
Chalky Teeth or Cheese Molars in Children
According to recent data, molar hypomineralisation (Chalky Teeth or Cheese Molars) is a common dental condition people experience globally. It is associated with dental problems that could adversely impact the patient’s quality of life. It also poses challenges to dentists in providing treatment options to their clients.
Molars affected by hypomineralisation are prone to post-eruptive enamel breakdown and caries. Childhood caries is a prevalent dental condition. It would help to diagnose and manage it as early as possible. Early diagnosis is essential for effective and conservative management. This paper highlights the various aspects of hypomineralised molars in children, including the available treatment options available.
What is Molar Hypomineralisation?
Hypomineralised molars refer to a developmental condition that affects teeth between the third trimester in pregnancy and the first four years of life, Brisbane kids dentist from Pure Dentistry says. The enamel in the affected teeth contains fewer minerals than the healthy teeth. The enamel becomes softer, and children with hypomineralised teeth complain of increased sensitivity, especially to cold or touch. The teeth are also more prone to decay than those not affected by the condition. The prevalence of hypomineralisation is on the increase, with up to 20% of the population in the UK being affected.
The teeth develop yellow or chalky white patches that make numbing for treatment difficult. Sometimes, the affected teeth are referred to as ‘cheesy’ molars. Although there is a difference in the enamel translucency of the hypomineralised teeth, there should be no changes in the thickness.


Will All Your Child's Teeth Be Affected?
It’s natural to worry about your child’s teeth when one of them is affected by hypomineralisation. In the primary teeth formation (milk teeth), the primary molars may become affected. When this happens, the chances are high that the child’s adult teeth will also have some form of hypomineralisation.
The condition commonly affects the first set of adult incisors and molars and is known as molar-incisor hypomineralisation (MIH). Biting forces cause the molars to break down quickly, but the incisors are only mildly affected. However, they create an aesthetic issue and may occasionally affect adult canines.
When to Consult a Dentist for Molar Hypomineralisation
If your child has molar hypomineralisation, dental check-up and clean and regular visits to the dentist and dental hygiene appointments are crucial. Fluoride applications are also essential to slow down the progression of the condition. During the dental visits, the dentist will remind you to help your child brush twice a day with fluoride toothpaste.
Taking care of your child’s hypomineralised molars can be challenging without the help of a dental professional. At Pure Dentistry, we understand this too well. This is why we offer to work with you and your child to help you take a proactive approach to manage MIH. For honest advice and reliable treatment options, contact us today for an initial consultation or book an appointment.
Preventing Management of Hypomineralised Molars
Hypomineralised molars are susceptible to acid attack and decay. Ensure to have your child’s diet assessed and get a recommendation for the proper dietary changes. If your child has difficulty brushing their teeth due to sensitivity, ensure they use a toothpaste containing fluoride to reduce caries.
Long-term use of products containing casein phosphopeptide amorphous calcium phosphate (CPP-ACP) is also an ideal preventative measure. The combined use of CPP-ACP and fluoride provides enhanced benefits than using either agent on its own. However, avoid CPP-ACP products in children with milk protein allergies due to the presence of casein.
Another effective preventive product is amorphous calcium phosphate, which contains substantial amounts of fluoride and ACP. These two are essential in enhancing remineralisation in the same way as 5,000 ppm fluoride products.
Another recommendation for preventive care is to fissure-seal the hypomineralised molars. When the enamel surface of MIH molars is intact, sealants containing resin can be used with an adhesive application before placement. This will increase the retention rate of the fissure sealant.

Extractions
Sometimes, a kids dentist will suggest extraction if there is crowding in your child’s mouth. They will remove the defective molars instead of the healthy teeth to create space and help the crowding. Extractions may also be necessary if the affected molars are chopped, broken, or cracked or if the nerves are affected by decay.
It’s essential to have an early orthodontic consultation to establish how to manage your child’s condition in the long term. If your child is young (between 6 and 8 years old), you may opt for one of the restorative options above. This is while waiting for the eruption of other permanent molars or until it is the right time for extraction. In the second phase of treatment, a general anesthetic (sleep dentistry for children) may be necessary.
Stainless Steel Crowns
Another treatment option is to install a pre-made silver crown to cover the entire affected tooth. This protects it from further damage from biting forces, decay, exposure to acid, and sensitivity. If your child’s teeth have visible defects and are chipped or broken, stainless steel crowns are the treatment of choice.
When properly placed, the crowns preserve the molars until adulthood until your child is ready for permanent dental crowns. Remember to have them replaced as your child grows older and the teeth continue to develop. When your child grows to adulthood, a dentist or prosthodontist will place permanent crowns in their gold or porcelain forms.
Adhesive White Sealants or Fillings
After treatment with fluoride-rich products, the dentist may place fillings. These will require constant monitoring and additional fillings as the enamel may continue to break off. Hypomineralised teeth that undergo filling and sealant treatments have over ten times more likelihood of requiring retreatment. The short lifespan of the fillings and the need for frequent treatment can be attributed to the weakness of the bond formed. It is also attributed to dental fear and anxiety that develops during the procedure.
Back Teeth Treatment Options
Back teeth can be as sensitive as the front teeth. Treatment options must also account for the extent of decay and how long the teeth are likely to last. Treatment options include:
- Fissure sealant
- White filling or stabilisation
- Stainless steel crown
- Tooth removal
Treatment Options Available
The treatment options the dentist recommends depends on how severe the clinical signs and symptoms are. An in-depth clinical examination and radiographs will help establish the most accurate diagnosis of your child’s MIH condition. Treatment also depends on whether the affected teeth are the front or back teeth.
If the teeth are overly sensitive, the dentist may recommend toothpaste with high fluoride content. Other options are a tooth mousse or regular fluoride varnish to lessen the sensitivity.
Diagnosis of Molar Hypomineralisation
The best time to diagnose MIH is when it appears to be apparent in either the primary or permanent teeth. Assessment is done on clean wet teeth, with the presentation varying depending on the severity of the condition. It ranges from yellow-brown opacities to white-creamy opacities. Other symptoms are post-eruptive enamel breakdown or atypical caries, or atypical restorations on at least one first primary molar.
The lesions should be larger than 1 mm to qualify as MIH. When this is the case, the doctor will ask you about any illnesses that occurred during pregnancy, during birth, or within the first three years of your child’s life. These are useful in supporting the diagnosis.
Clinical manifestations
Hypomineralisation causes the enamel to become softer as it contains up to 21% less mineral. This exposes it to breakages under regular biting forces. Filling the resulting gap with the relevant materials is difficult because the bonding created is weak. Therefore, fillings fall off, and new decay can form quickly at the edges.
Besides, the enamel of the affected teeth is highly porous and hence also very sensitive. One sign that this is the case is when your child constantly avoids hot or cold foods. In other instances, they can’t brush their teeth thoroughly due to high levels of sensitivity. The sensitivity interferes with numbing, which makes the child feel pain during dental procedures like drilling.
A child affected by hypomineralisation develops extreme dental anxiety whenever they have to undergo dental work at a young age. With time, cosmetic concerns also arise, especially where the front teeth are affected by developmental defects.
Causes of Molar Hypomineralisation
The causes of molar hypomineralisation are still unclear, but some factors may be responsible in the first four years of life. Exposure to environmental pollutants during the last trimester and early life is a contributing factor. Children with prenatal, perinatal, or postnatal problems also tend to have more teeth affected in increasing order.
Literature also suggests other possible causes like oxygen starvation, low birth weight, and genetic factors. Some studies show the possibility of a genetic role in the formation of MIH. A genetic variation may cause an interaction that leads to MIH. The use of antibiotics during pregnancy and severe illnesses during the first few years after birth are other disturbances that cause the condition. Others include coughs, colds and fever. Sometimes, it can occur without any known reason.


























